
Health plans are heading into 2026 with a mix of confidence and uncertainty. Regulatory pressure is rising, administrative costs remain high, and member and provider expectations keep increasing.
Deloitte’s 2026 US Health Care Outlook highlights three strategies healthcare leaders are prioritizing:
-
empower consumer health with digital experiences and technology
-
scale generative AI and agentic AI to modernize operations across all functions
-
join forces with other industries to unlock innovation and impact
At Productive Edge, we view this as validation of the shift we’ve been working on with payer clients for the last few years: moving from AI experiments to operational modernization.
But there’s a key detail that determines whether this shift succeeds or stalls.
In payer operations, the real bottleneck isn’t the AI model.
It’s the fact that critical business logic still lives in documents.
The payer reality: the rules of the business are trapped in PDFs
In most health plans, the “source of truth” for decisions lives in places like:
-
medical policies
-
clinical criteria
-
provider manuals
-
authorization guidelines
-
benefit documents
-
regulatory guidance
-
internal SOPs and job aids
And most of it is still stored and distributed as PDFs.
That creates a structural problem:
If your policies and criteria are not machine-readable, your workflow can’t be fully machine-executable.
So even if you introduce AI, you still end up with:
-
inconsistent decisions
-
slow turnaround times
-
heavy manual review
-
difficulty proving compliance
-
constant rework and escalation
This is why payers can run pilots forever and still struggle to scale.
The “document types” unlock: convert policy PDFs into machine-readable decision logic
When we talk about document types, we’re not talking about classification for its own sake.
The highest-value document type in payer operations is the policy.
Because policy documents contain:
-
the rules
-
the exceptions
-
the decision criteria
-
the rationale requirements
-
the documentation requirements
-
the “if/then” logic that drives outcomes
So the unlock is:
Step 1: Extract rules from policy documents (even if they start as PDFs)
This means turning policy language into structured components like:
-
conditions
-
thresholds
-
required evidence
-
exclusions
-
timing constraints
-
dependencies (e.g., prior therapies tried, diagnosis confirmed)
Step 2: Build a decision model that is explicit and testable
Once rules are structured, you can lay them out into a decision model so the plan can:
-
apply the same logic every time
-
validate outcomes
-
identify gaps in evidence
-
support reviewers with traceable rationale
Step 3: Connect the decision model to the business process
This is the missing link in most AI projects.
It’s not enough to recommend a decision.
You need to connect the logic to workflow steps like:
-
intake and triage
-
evidence gathering
-
criteria matching
-
routing and exception handling
-
documentation generation
-
communications
-
audit trail creation
That’s how you arrive at the same decision twice, in a predictable and compliant way.
And it’s where agentic AI becomes operational.
Why this matters now: prior authorization modernization is becoming mandatory
Deloitte calls out prior authorization as a major operational bottleneck and highlights the impact of new CMS requirements tightening timelines and increasing transparency.
This is exactly the kind of workflow where machine-readable policy and decision logic becomes essential.
Because prior auth isn’t just a document problem. It’s a rules problem.
Health plans are expected to be faster and more consistent, while also being able to prove:
-
decisions were grounded in policy
-
criteria were applied correctly
-
rationale was documented
-
processes were compliant
That combination (speed, repeatability, and compliance) is hard to achieve with manual review at scale.
What “agentic AI” should mean for payers (in plain terms)
A lot of AI talk in healthcare focuses on summarization and drafting. That’s useful, but it doesn’t change the operating model.
Agentic AI is different because it can execute across workflows.
For payers, that means AI agents that can:
-
ingest incoming documents (fax, portal, attachments, clinical notes)
-
identify what policy applies
-
map evidence to criteria
-
determine what’s missing
-
recommend next-best actions
-
route work correctly
-
generate compliant documentation
-
maintain traceability and audit trails
But none of that scales unless the policy logic is machine-readable.
How Productive Edge approaches payer AI: modernize workflows without forcing rip-and-replace
Our focus isn’t simply “add AI to a process.”
It’s helping payers modernize workflows so decisions can be made consistently, predictably, transparently, and compliantly.
But we also recognize an important reality: not every payer wants (or needs) to tear down and rebuild their workflows from scratch.
That’s why we typically assess two paths with clients:
Option 1: Surround and supercharge the existing workflow with AI
This approach keeps the current workflow structure in place, but adds AI to reduce friction and improve speed and quality, for example:
-
extracting evidence from documents
-
mapping evidence to policy criteria
-
automating documentation and communications
-
improving routing and exception handling
-
strengthening audit trails and compliance traceability
Option 2: Rewire and reimagine the workflow with AI
This approach redesigns the workflow end-to-end around machine-readable policy logic, decision models, and agentic execution. It’s best when current processes are too slow, inconsistent, or expensive to scale.
In both cases, the foundation is the same:
-
unlock rules from policy documents
-
formalize them into decision models
-
connect decision logic to workflow execution across systems
-
include human oversight where required
-
build governance and traceability from day one
That’s how you modernize utilization management and authorization operations without forcing a rip-and-replace transformation.
What payers should take from Deloitte’s 2026 outlook
Deloitte is right: scaling generative AI and agentic AI is a 2026 priority.
But the practical payer takeaway is this:
Scaling agentic AI depends on converting policy documents into machine-readable decision logic.
That’s what makes decisions repeatable.
That’s what makes workflows predictable.
That’s what makes compliance provable.
And that’s what separates AI that demos well from AI that actually runs payer operations.
Want to see how we help payers organize and scale AI adoption?
One more point Deloitte’s report reinforces indirectly: scaling AI isn’t just a technology challenge. It’s an operating challenge.
Most payers aren’t pursuing five use cases. They’re pursuing 50, 100, or more across UM, claims, service, care management, and compliance. Without a clear system for intake, assessment, prioritization, and governance, AI efforts quickly become fragmented, duplicative, and hard to scale.
Productive Edge uses a structured methodology for enterprise AI adoption that starts with intake and prioritization and leads into delivery of high-impact workflows like prior authorization and utilization management.
As part of this approach, we provide an AI Portfolio Manager tool that serves as a command center for enterprise AI adoption.
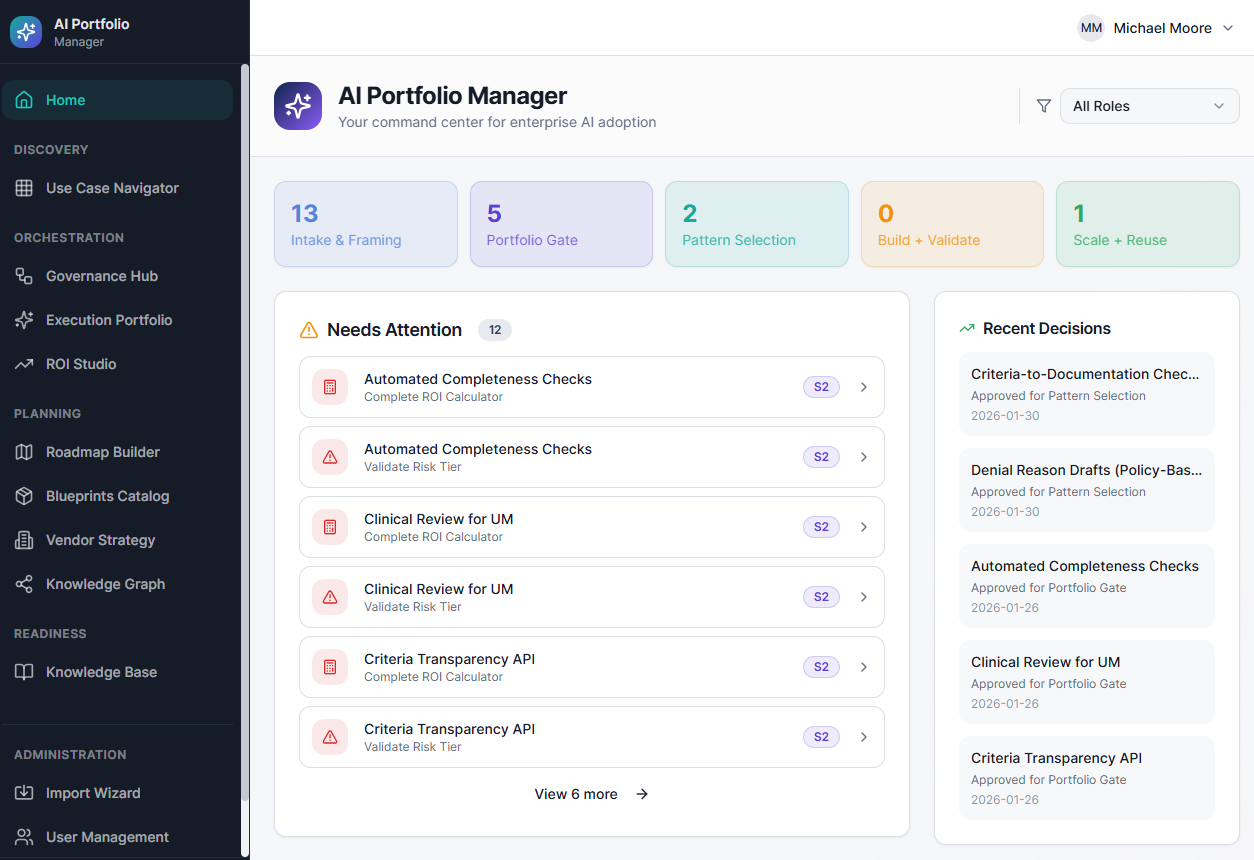
It helps payer teams manage the full lifecycle of AI initiatives, including:
-
use case intake
-
assessment and feasibility scoring
-
prioritization and roadmap planning
-
value tracking and governance
We include the AI Portfolio Manager in our engagements.
If you’d like, we can walk you through the tool and show how it helps payer organizations bring order to hundreds of AI ideas and focus execution on the few that actually drive measurable operational impact. Contact us to schedule a walkthrough.




